Don’t miss Black Poppy’s unique hard copy magazine -available now and posted to anywhere in the world. Catch up on the latest news, views and lifestyle issues with one of the worlds best loved drug user magazines; exclusively created and produced by users for users. If drugs influence your lifestyle – then you need BP magazine for the latest news, stories and articles on drug use. Click here for more info on the mag and whats inside.
I know its been ages since we wrote but today, well, a cuple of crew members had such a marvellous day – just punching out into the bewildering and joyous balloon that encompasses us when we get really fucking high! When we have such a fabulous time, and share such meaningful heartfelt, and soulful moments with our loved drug buddies…that it seems such a crime to not shout to the world occasionally, “Fucking Jeezus, it can be such fun to get high!”
We dont celebrate that fact enough and I for one want to shout out to all our people worldwide today, that yeh! We dig it, and with all the pain that can come with our drugging journeys, there are some highs that honestly can make you feel sorry for all the straights in the world who never get to have their brain’s inner ‘barriers’ come down; when our ‘Doors of Perception’ open up to us and allow us into areas of the heart and soul that are so amazingly joyous, so connected, so at peace with the whole of humanity that folks, there are simply no words to express it!
Set, Setting and Good Intentions
Today, my partner and I put on some sounds, had a David Attenborough planet doco on for some beautiful visuals, and had one of the most incredibly loving afternoons either of us have ever had in our lives!
Somehow, we chose the Fleetwood Mac album ‘Rumours’ almost as a fill in choice while we were connecting up all the tech in preparation for the afternoon ‘event’ (as the more experienced of us get to REALLY appreciate – it is ALL about the ‘Set and Setting to get the most out of your substance of choice) . But then, the drug (ketamine, at this stage) started enveloping the room and as the tunes began to create the ambiance, we began to weave into each others arms, then hearts. Fully blissed out by our embrace, we fell into a realm where the real, raw human emotion of love – a place that sits deep in the soul, opened up. That depth of loving, was so overwhelming in its humanity, its kindness, it’s intimacy and it’s shared protection that it was indescribable in its realness of feeling. You are as one, yet you are so aware of each other individually, it literally felt like we touched each others very hearts, through the very prisim of our souls, and so also understood our minds!..Well, then Songbird came on and so did the the second wave of Kay, and we just stayed in these loving realms that were just……too fucking beautiful for words!
Let’s Celebrate!
And I thought, and then said to my partner, “wow, you know we dont celebrate the gifts that drugs can give us, enough. We speak the language of either minimising harm’s and staying safe while out there ‘knocking shoulders with the black market’ or, we see the social media mashups of people getting smashed, overdoing it, overdosing and the like. But, as I mentioned before, in-between those days of brutal pain and struggle some of us certainly endure at times, we are also given access to such great heights, it is why we do indeed keep going, despite those lows that occur. There are highs that bestow us with such clarity, love, sheer fun and hilarity and such joy that, well, it seems wrong not to just say it outloud sometimes – “Goddamit, we take drugs for a REASON – and that’s coz we like them, they really do offer us access to experiences that are so incredible, so comforting, so shudderingly ethereal that we should really be able to talk about them more. Yes it might be dodgy territory considering the risks involved in turning a newbie on to drugs by talking them up, but if we talked about how to make the most of them, how to properly prepare your substances and – the many ways of preparing your environment- you can get a much more fulfilling and life enhancing experience, ones that are often naturally safer anyway.
International Drug Users Day, November 1st.
So I just wanted to say to y’all, that our staunch and incredibly charistmatic user activist hero, Theo Van Dam, from Amsterdam/Netherlands, actually created a day, some years back (that still endures today) called International Drug Users Day. A day for US, where we can hold our heads high (no pun intended) come out of our prohibition created closet and celebrate our culture – our journeys, our lives, our friends, lovers and today, our global activist community who continue to work day in, day out to educate, agitate and care for those of us struggling to survive under the collateral damage of prohibition and the sheer ignorance and discrimination it creates.
It is to celebrate a culture that has evolved and been inspired by more than sheer talent, psychic exploration and a good helping of decadence and hedonism, it is also those beautiful, intimate days, times we have spent with our friends and lovers that are special in ways it is hard to find the words to express it…although we come very close, as we sing, dance, paint, and create the kind of artistic expression that go on to influence the cultures of the world. We do indeed have a culture. And it should be celebrated. November 1st comrades, November 1st. What will YOU be doing come this November?
It is our day to revel in our own culture, our brilliance, our friendships, loves and the goddamn courage it can take to go through what we do (in this global War on People who Use Drugs). It is on November 1st, comrades. We know what we will be doing…
(Just be careful of the fireworks lol!)
Dedicated to Theo Van Dam, Dutch Activist made of the Real Stuff, inventor of International Drug User Day, November 1st.
Us oldies know all about it, I need say no more that this headline… But yet there is more to say, quite a bit more. And this peer to peer project - containing the news and views and research deep dives - all which would be nothing without your input and your upfront honesty u generously share here -.has brought a couple members of our BP crew, deeply distressed to our blog, needing to share, but wanting to ask our injecting comrades their best advice….
The point is – when u are fishing, and by fishing we mean for a vein, one of your last, sad, tiny, sore delicate veins, to puncture, rewards us hopefully, and, often leave us sore, swollen, red, lumpy…. You know what we mean friends….
We wanna know from all of u out there, what is the best after/post injection cream you use, to decrease the swelling, cool down the heat, prevent the scarring…. What do u use? C’mon, we want answers from across the globe here as we all do it, have done it at some stage in our lives!
BP has a few suggestions to start us off.
100% Aloe Vera Gel/cream:
You cannot beat 100% Aloe Vera Gel for rubbing all over your arms and legs – avoid open sores but rub all over like hand cream. A cuple times a day. I imagine even a leafs juices would work, bit man is it effective! Especially to reduce the redness and swelling!
2) Hirudoid Cream or Gel – under £ 5 from most chemists.
Hirudoid Cream or gel
This is the business. If u have a screaming red bump, without a big open hole, this will have it down overnight we reckon. It is a. MUST. in ones medicine cabinet, read on….
“Hirudoid is indicated for the treatment of superficial thrombophlebitis and the soothing relief of superficial bruising and haematoma. ” Similar stuff they use for hemorrhoids dudes, it’s reduces inflammation. Almost straight away, and is fabulous for hands arms and legs, but no big holes- u need the doc for that sugar. They even give this out as standard in Aussie and Kiwi needle exchange packs, and they all swear by it.
Vitamin E cream; cheap!
Always. Always. Always the biz to reduce scarring and prevent scarring occurring. In oil or cream, use it regularly, even on old tracks, and u won’t be disappointed, we promise. Another for the medicine cabinet friends.
Calendula often mixed with witch hazel.. under £10
Started out using this and was blown away by how good it work. Again not on open sores but anywhere red and swollen,. Places u have missed, overused, etc. Either herbal stuff is great but both are brilliant.
We will keep thinking friends but please,. Comment below and we will add them to this article
We wanna know what u do about this desperately upsetting dilema. Later we will discuss why we do it when it’s obviously so…. Painful. We don’t think it’s addiction to the needle either. Things are more complicated than that. Let us know whatcha think friends, and let’s get some ideas for our comrades in (sore) arms. …. Take care out there. BP
I wanted to share this very interesting article from last year, which talks about the recent race pharmaceutical companies have been in to get the first ketamine based anti depression product into the market, which many BP readers may already know.
Well, in case you missed the fairly quiet news, which is actually big news, but which you could be forgiven for not seeing as it didn’t make much of a splash – especially considering the rather large fact that many of us are still getting locked up on a regular basis in prisons around the world for using our own Kay for our own self medication and self…exploration…But I digress, I want to pass on this news you just might have missed…
Ketamine, or rather, ‘esketamine in the nasal spray formulation called Spravato’ (‘dig the hipster parlance’ as my buddy used to say!) has finally made it out the door first, as a proper polished big pharma product- via the company Janssen Pharmaceuticals (a subsidiary of Johnson and Johnson). Guess we should say thanks or something…
Anyhoo, that has made ketamine “the first novel depression drug to hit the market in more than 50 years.” Now that IS big news isn’t it? Yay Kay! So it was officially approved by the US FDA in March 2019 and it appears everyone has big hopes for it.
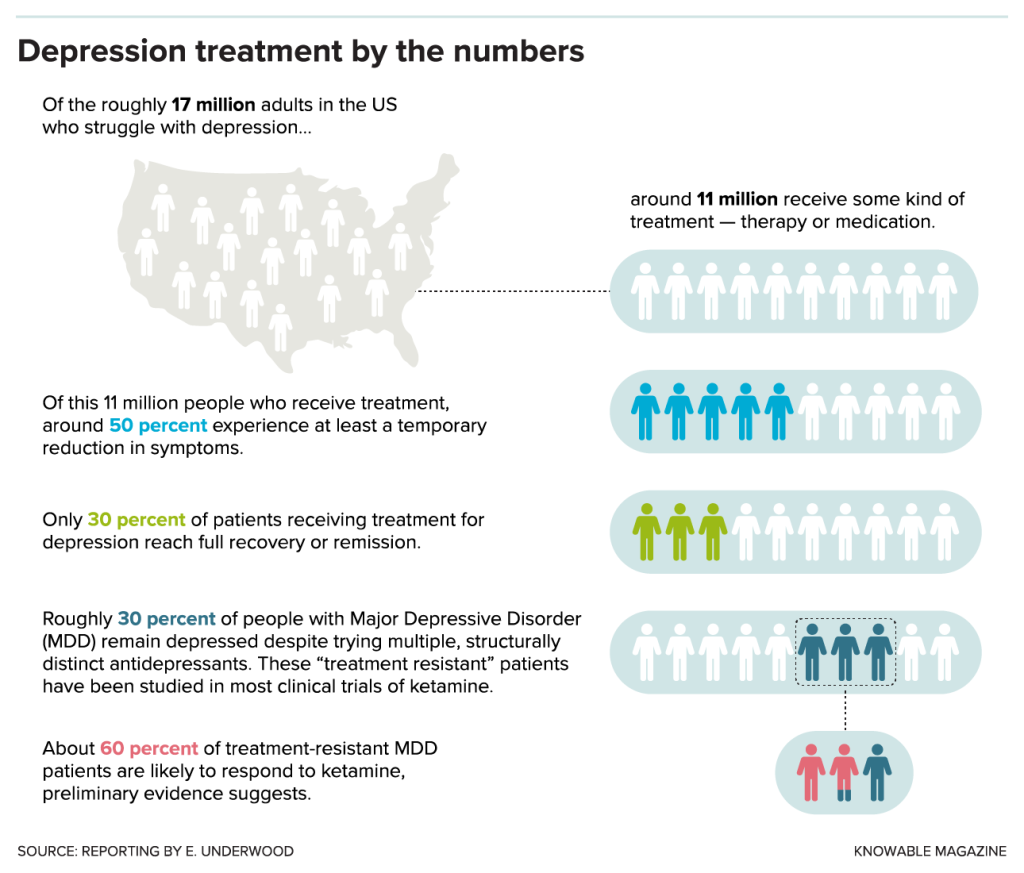
In brief, and from what I can gather, the idea is to prescribe it to those suffering severely with depression and suicide ideations – along with a common antidepressant; being dosed nasally a couple of times a week for 4 weeks, and then being reassessed as to whether your prescription should contine. But it’s expensive…of course. Thanks again guys…we think?
And if you are interested in a little more information on dosing, which to be honest, we DO want to know how much the dose is (and yeh, they are super small) along with prescribing information and stuff like that, I have included a couple of links that shed a bit more light on this fascinating subject, that many BP readers will be very interested in, indeed. One more thing to add, there are also a whole heap of intravenous ketamine clinics popping up throughout the USA, giving teeny tiny doses of Kay, IV, as you lie flat out on a trolley bed in a therapists office for an hour or so, before you feel better and they send you on your way with your next appointment in hand. And what results they have had! Really very good readers, though we might suspect as much. The malleability of ketamine makes it an ideal drug to ‘guide’ and I am certain one could address numerous issues and feelings of depression from using it in a…therapeutic kind of way. Anyway, read on, the article is very interesting and the subject well worth a further bit of study, friends. Adiós til next time. EO.
Listening to Ketamine, The terrific article below was written by Emily Underwood, April 2019, updated in 2020, from Knowable Magazine.
At 32, Raquel Bennett was looking for a reason to live. She’d struggled with severe depression for more than a decade, trying multiple antidepressants and years of talk therapy. The treatment helped, but not enough to make it seem worth living with a debilitating mental illness, she says. “I was desperate.”
In 2002, following a friend’s suggestion, Bennett received an injection of ketamine, an anesthetic and psychedelic party drug also known as Special K. During her first ketamine trip, Bennett hallucinated that God inserted a giant golden key into her ear, turning on her brain. “It was as if I was living in a dark house and suddenly the lights came on,” she says. “Suddenly everything seemed illuminated.”
The drug lifted Bennett’s depression and dispelled her thoughts of suicide within minutes. The effect lasted for several months, and, she says, the respite saved her life. She was fascinated by the drug’s rapid effects and went on to earn a doctoral degree in psychology, writing her dissertation about ketamine. Today, she works at a clinic in Berkeley, California, that specializes in using ketamine to treat depression. “This medicine works differently and better than any other medication I’ve tried,” she says.
When Bennett experimented with ketamine, the notion of using a psychedelic rave drug for depression was still decidedly fringe. Since the first clinical trials in the early 2000s, however, dozens of studies have shown that a low dose of ketamine delivered via IV can relieve the symptoms of depression, including thoughts of suicide, within hours.
Even a low dose can have intense side effects, such as the sensation of being outside one’s body, vivid hallucinations, confusion, and nausea. The antidepressant effects of ketamine typically don’t last more than a week or two. But the drug appears to work where no others have — in the roughly 30 percent of people with major depression who, like Bennett, don’t respond to other treatments. It also works fast, a major advantage for suicidal patients who can’t wait weeks for traditional antidepressants to kick in.
“When you prescribe Prozac, you have to convince people that it’s worth taking a medication for several weeks,” says John Krystal, a psychiatrist and neuroscientist at Yale University in New Haven, Connecticut. “With ketamine, patients may feel better that day, or by the next morning.”
The buzz around ketamine can drown out just how little is known about the drug. In the April 2017 JAMA Psychiatry, the American Psychiatric Association published an analysis of the evidence for ketamine treatment noting that there are few published data on the safety of repeated use, although studies of ketamine abusers — who typically use much higher doses — show that the drug can cause memory loss and bladder damage.
Most clinical trials of the low dose used for depression have looked at only a single dose, following up on patients for just a week or two, so scientists don’t know if it’s safe to take the drug repeatedly over long periods. But that’s exactly what might be necessary to keep depression at bay.
The analysis also warned about ketamine’s well-established potential for abuse. Used recreationally, large doses of the drug are known to be addictive — there’s some evidence that ketamine can bind to opioid receptors, raising alarms that even low doses could lead to dependence. (BP Ed – that is interesting.)
Bennett has now been receiving regular ketamine injections for 17 years, with few negative side effects, she says. She doesn’t consider herself addicted to ketamine because she feels no desire to take it between scheduled appointments. But she does feel dependent on the drug, in the same way that a person with high blood pressure takes medication for hypertension, she says.
Still, she acknowledges what most clinicians and researchers contend: There simply aren’t enough data to know what the optimal dose for depression is, who is most likely to benefit from ketamine treatment, and what long-term treatment should look like. “There’s a lot that we don’t know about how to use this tool,” Bennett says. “What’s the best dose? What’s the best route of administration? How frequently do you give ketamine treatment? What does maintenance look like? Is it OK to use this in an ongoing way?”Despite the unknowns, pharmaceutical companies have been racing to bring the first ketamine-based antidepressant to market. In March, the U.S. Food and Drug Administration approved a ketamine-derived nasal spray, esketamine, developed by Janssen Pharmaceuticals, a subsidiary of Johnson & Johnson.
Only two of Janssen’s five phase III trials had shown a benefit greater than taking a placebo. Still, in February an independent panel recommended FDA approval. That makes ketamine the first novel depression drug to hit the market in more than 50 years, notes Carlos Zarate Jr., a psychiatrist who studies mood disorder therapies at the National Institute of Mental Health.
Although clinicians are hopeful that Janssen Pharmaceutical’s newly approved esketamine nasal spray, Spravato, will expand access to treatment, many also worry about the drug’s potential for abuse.
Thousands of people are already flocking to private clinics like Bennett’s, which provide intravenous ketamine infusions. Because the drug was approved in the 1970s as an anesthetic, physicians can legally provide the drug as an “off-label” depression treatment. Many ketamine clinics have long waiting lists or are so swamped that they aren’t accepting new patients, and Janssen’s nasal spray could rapidly expand access to treatment.
But some researchers worry that the nasal spray won’t solve many of ketamine’s problems and could create new ones. Although the FDA is requiring that the nasal spray be administered only in a certified doctor’s office or clinic, esketamine is “every bit as habit forming as regular ketamine,” and will be difficult to keep out of the hands of abusers, says Scott Thompson, a neuroscientist at the University of Maryland and a coauthor with Zarate of a 2019 review on fast-acting antidepressants in the Annual Review of Pharmacology and Toxicology. A nasal spray can’t deliver as precise a dose as an IV infusion, Thompson notes. “If someone has got a cold, they’re not going to get the same dose.”
Scott Thompson of the University of Maryland discusses how ketamine is changing the landscape of the psychiatric treatment of severe depression. Video Produced by Hunni Media for Knowable In Thompson’s view, esketamine holds few advantages over generic ketamine, which costs less than a dollar per dose, although the IV infusions in private clinics often cost hundreds of dollars per visit. Janssen has indicated that each esketamine treatment will range from $590 to $885, not including the costs of administration and observation.
Zarate and others are still thrilled to see big pharma investing in ketamine, after decades of stalled efforts to find new psychiatric drugs. “As esketamine hits the market, venture capitalists will come up with better versions and move the field forward,” Zarate says. Several drug companies are now testing other ketamine-like compounds in hopes of developing drugs that have its potent antidepressant potential without its psychedelic and dissociative side effects.
Some researchers are also testing whether ketamine works for conditions beyond depression, such as obsessive-compulsive disorder, as well as in specific subsets of patients, such as severely depressed teenagers. Other scientists are using ketamine to help untangle one of the biggest mysteries in neuroscience: What causes depression?
Seeking Answers in Neural Wiring.
Thirty years ago, the prevailing thought was that low levels of certain brain chemicals, such as serotonin, caused depression. Boosting those could remove symptoms.
“I felt that depression needed months or weeks of treatment — that the plastic changes involved in the healing process would require weeks to reset themselves,” says Todd Gould, a neuropharmacologist at the University of Maryland and a coauthor of the recent review paper. But ketamine’s speed of action casts doubt on that idea.
Newer evidence suggests that depression is caused by problems in the neural circuits that regulate mood, Gould notes. Much of the evidence for this faulty-wiring hypothesis comes from rodents. Starting in the 1990s, scientists began to discover intriguing abnormalities in the brains of mice and rats that had been exposed to certain stressors, such as bullying by a big, aggressive male.
Stress and trauma are strong predictors of depression in people, but scientists can’t ask rats or mice if they are depressed. Instead, they use behavioral tests for classic depression symptoms such as anhedonia, the inability to take joy in pleasurable activities, Thompson says. Depressed animals “give up easily” in experiments that test their willingness to work for rewards like sugar water, or their interest in the intoxicating scent of a potential mate’s urine. “They can’t be bothered to cross the cage,” he says.
Thompson and others have found that there are fewer connections, or synapses, between neurons that communicate reward signals in the brain in depressed animals. Other labs have found shriveled connections in neuronal circuits key to decision-making, attention, and memory. Brain imaging studies in people with depression have also revealed abnormal activity in neural circuits that regulate emotion, suggesting that the findings in rodents may also apply to humans.
If faulty neural connections are to blame for depression, the next question is, “How do we get atrophied neural pathways to regrow?” Krystal says.
Circuit training The answer, many scientists now believe, is the brain’s most abundant neurotransmitter, glutamate.
Glutamate is the workhorse of the brain. It relays fleeting thoughts and feelings, and enables the formation of memories by strengthening synaptic connections. Glutamate is the reason you can still ride a bike years after you learned, even if you never practiced.
Not all glutamate activity is good. Too much can cause the equivalent of an electrical storm in the brain — a seizure — and chronically high levels may lead to dementia. Abnormalities in glutamate receptors — specialized proteins on the surface of brain cells where glutamate can dock and bind — are linked to a wide array of psychiatric diseases, including depression and schizophrenia.
To maintain balance, cells called inhibitory interneurons act like brakes, releasing a neurotransmitter called GABA that quiets brain activity. Most mind-altering drugs work by changing the balance between GABA and glutamate — amphetamines and PCP enhance glutamate signaling, for example, while alcohol inhibits glutamate and boosts GABA.
By the 1990s, scientists had discovered that ketamine triggers a gush of glutamate in the brain’s prefrontal cortex. This region governs attention and plays an important role in emotional regulation. The out-of-body sensations that some people experience when they take ketamine may occur because this rapid release of glutamate “excites the heck out of a whole bunch of neurons” in the prefrontal cortex, says Bita Moghaddam, a neuroscientist at Oregon Health & Science University who discovered the drug’s glutamate-revving effect on rats while studying schizophrenia.
Scientists aren’t sure yet how ketamine forms stronger neural circuits. But the hypothesis goes roughly like this: When ketamine enters the brain, it causes a short-term burst of neuronal activity that triggers a series of biochemical reactions that create stronger, more plentiful synaptic connections between brain cells.
At first, many researchers thought ketamine’s antidepressant effects relied on a structure located on the surface of neurons, called the NMDA receptor. Like a key that fits into different locks, ketamine can bind to several types of NMDA receptor, making neurons release the excitatory glutamate neurotransmitter.
This hypothesis suffered a blow, however, when several drugs designed to bind to the NMDA receptor (as ketamine does) failed in clinical trials for depression.
Illustration of an NMDA receptor Central to the controversy over how ketamine works in the brain is the NMDA receptor (illustrated here), which binds to the neurotransmitter glutamate. Some scientists believe ketamine’s antidepressant effects hinge on its ability to block NMDA receptors, but others believe the drug works via other mechanisms. Resolving that mystery is key to developing similar drugs with fewer side effects, scientists say. Furukawa Lab, CSHL Esketamine also complicates the story. Ketamine is made up of two molecules that form mirror images of each other, R- and S-ketamine. Esketamine is made up of just the S form and binds roughly four times as effectively as R-ketamine to the NMDA receptor. Despite acting much more powerfully on the NMDA receptor, studies in rodents suggest that S-ketamine is a less potent antidepressant than R-ketamine, although it’s not yet clear whether or not R-ketamine could work better in humans.
Zarate and others now believe ketamine may work through a different receptor that binds glutamate, called AMPA. By pinpointing which receptor ketamine acts on, researchers hope to develop a similar drug with fewer side effects. One hot lead is a compound called hydroxynorketamine (HNK) — a metabolic byproduct of ketamine that does not affect NMDA receptors but still produces rapid antidepressant effects in rodents. The drug appears to lack ketamine’s disorienting side effects, and Zarate and Gould plan to launch the first small clinical trials to establish HNK’s safety in humans this year, likely in around 70 people. “I think we have a very good drug candidate,” Gould says. (Zarate and Gould, among others, have disclosed that they are listed on patents for HNK, so they stand to share in any future royalties received by their employers.)
Plastic synaptic remodelers To alter how the brain processes mood, scientists believe ketamine must ultimately change synapses. In experiments in rodents, Ron Duman of Yale University has shown that both ketamine and HNK can harness one of the brain’s most important tools for synaptic remodeling: brain-derived neurotrophic factor, or BDNF.
BDNF is a protein intimately involved in shaping synapses during brain development and throughout the lifespan. Healthy brain function depends on having just the right amount of BDNF in the right place at the right time. Many mental illnesses, including depression, are associated with low or abnormal amounts of the protein. For example, samples of brain tissue from people who have died by suicide often contain abnormally low amounts of BDNF.
Duman and colleagues have found that both ketamine and HNK cause a sharp uptick in the amount of BDNF that is released from neurons. This increase is required for the drugs’ antidepressant effects, and for the increase in dendritic spines — the stubby protrusions that form synaptic connections with other neurons. Both ketamine and HNK also seem to reduce inflammation, which has been linked repeatedly to the stress-induced loss of synapses.
Compared with a control, a rat neuron (in red) treated with ketamine has grown more dendritic spines (shown by yellow arrows). Ketamine strengthens connections between brain cells. Compared with a control (top), a rat neuron (red) treated with ketamine (bottom) has grown more dendritic spines (shown by yellow arrows). Rong-Jian Liu, George Aghajanian & Ronald S. Duman Ketamine is not the only compound that can induce rapid synaptic plasticity: Other psychedelics, such as ecstasy (MDMA), acid (LSD), and DMT also trigger similar structural changes in neurons and rapid antidepressant effects in rodents, researchers at the University of California at Davis recently found. The effects don’t hinge on getting high, the team reported in March in ACS Chemical Neuroscience. Even very small doses — too low to cause perceptual distortions — can increase synapse density and lift depression.
Traditional antidepressants such as Prozac also increase BDNF levels in the brain, but not nearly as fast as ketamine does, Duman says. That is why most antidepressants take so long to remodel synapses and relieve depression symptoms, he says.
Dissecting depression Beyond promising new treatments, Zarate and other researchers see ketamine as a powerful tool for probing depression’s tangled neurobiology. Studies in mice and rats are a good start, but scientists need to study the drug in people to truly understand how ketamine affects the brain. Unlike traditional, slower-acting antidepressants, ketamine lends itself to short-term lab experiments.
Zarate is using neuroimaging tools such as fMRI to study the human brain on ketamine. Past studies have shown that in people with depression, communication among several key brain networks is disrupted. One network, called the default-mode network (DMN), is involved in self-referential thoughts such as ruminating about one’s problems or flaws. This network tends to be hyperactive in people with depression, and less connected to more outwardly attuned brain networks such as the salience network, which helps the brain notice and respond to its surroundings.
Neural activity prior to a ketamine infusion (on the left) and six to nine hours after an infusion (on the right). Ketamine appears to strengthen connections between neural networks in people with severe depression. In a study comparing neural activity prior to a ketamine infusion (left) and six to nine hours after an infusion (right), a single dose made the brain more responsive to a simple sensory stimulus, the light stroking of a finger. Carlos Zarate & Jessica Gilbert, Experimental Therapeutics and Pathophysiology Branch (ETPB), National Institute of Mental Health (NIMH) In one recent study, Zarate and his colleagues found that after receiving an IV dose of ketamine, people with depression had more normal activity in the default mode network, and that it was better connected to the salience network. At least temporarily, the drug seems to help people get unstuck from patterns of brain activity associated with repetitive, negative thoughts. Zarate does caution that the study results need to be replicated.
The team has also used brain imaging to study how ketamine affects suicidal thoughts. About four hours after an infusion of ketamine, a chunk of the prefrontal cortex that is hyperactive in people with depression had calmed down, researchers found, which correlated with people reporting fewer thoughts of suicide.
Ketamine also seems to tune other brain regions that are key to effective treatment. Last year, scientists published a study in mice showing that ketamine quiets abnormal activity in the lateral habenula, a small nodule wedged deep under the cortex. Some researchers have described the lateral habenula as the brain’s “disappointment center.” The region is responsible for learning from negative experiences, and is hyperactive in people with depression, as if “broadcasting negative feelings and thoughts,” Thompson says.
Such studies remain exploratory. As to why ketamine works — and just as important, why its effects are transient — scientists are still speculating. “I think ketamine is resetting neural circuits in a way that improves the symptoms of depression, but the risk factors — whether genetic, environmental, or other risk factors — are still present,” Gould says. “It seems to help reset things temporarily, but the underlying cause is not necessarily resolved.”
Helen Mayberg, a neurologist at Mount Sinai Hospital in New York who specializes in using an experimental procedure called deep brain stimulation to treat depression, suggests that ketamine may be like using a defibrillator on someone experiencing cardiac arrhythmia. “I am not addressing the fact that you have underlying heart disease, but now that your arrhythmia is gone, I can concentrate on other treatments.”
It’s important to put the potential risks of ketamine into perspective, particularly for people contemplating suicide, researchers emphasize. Most people are willing to tolerate severe side effects for other life-saving treatments, such as cancer drugs, Mayberg points out. “If you can interrupt an extreme suicidal plan and ideation, I’ll take that.”
Ketamine in teens? For Krystal, weighing ketamine’s still largely uncharted risks and potential rewards ultimately comes down to a deeply personal question: “What would we want for ourselves? For our families? Do we want them to have to go through several failed trials over several months, or even a year, before taking a medication that might make their depression better in 24 hours?”
Some of the hardest decisions are likely to involve children and adolescents. Hospitalization for youth suicide attempts and ideation nearly doubled between 2008 and 2015, leaving many clinicians — and parents — desperate for more effective and rapid treatments. Left untreated, depression is “really bad for the brain” and can cause serious, long-term cognitive and developmental problems when it starts young, Zarate says. “The question is, is that going to be better than the long-term side effects of ketamine?”
Untreated depression is really bad for the brain, especially in the young. The question is, is that going to be better than the long-term side effects of ketamine?
Scientists don’t yet know. Ketamine has been deemed safe to use as an anesthetic in children, but there aren’t yet sufficient clinical data to show how low, repeated doses of ketamine used for depression could affect the developing brain.
On a more fundamental level, scientists don’t fully understand the neurobiology of adolescent depression, notes psychiatrist Kathryn Cullen of the University of Minnesota. It may involve abnormalities in brain development, such as the way the prefrontal cortex connects to brain regions that process emotion, but “we don’t know if the brain connection abnormalities emerge because of toxic stress induced by depression, or if these abnormalities predispose people to develop depression, or if depression itself reflects abnormal development,” Cullen says. “It’s critical to figure out how to alleviate the biological changes that are associated with [teen] depression so that the brain can get back on a healthy trajectory.”
Two recent clinical trials — one at Yale and another at Minnesota run by Cullen — have found that ketamine can lower symptoms in severely depressed teenagers, but neither study was set up to follow the teenagers long-term, says Cullen. Janssen is currently running a trial of its esketamine nasal spray with 145 youths who are suicidal, but the results of that study have not been published yet. Cullen thinks ketamine has potential for use in teens, particularly to avoid suicide, but “there are still a lot of unknowns.”
Not just a quick fix Worldwide, depression afflicts more than 300 million people, making it the leading global cause of disability. When contemplating such overwhelming misery, the vision of a world in which depression can be cured with a single injection or squirt of nasal spray holds obvious appeal.
But — despite the hype — that is not what ketamine offers, Bennett says. Based on her own experience as a patient, and her clinical work, she is troubled by the framing of ketamine as a “rapid” depression treatment if that precludes the slower, more effortful process of psychotherapy. Without psychotherapy, she says, “you’re not giving patients any tools to help themselves, just making them dependent on a molecule that has temporary effects. When the effect wears off, they have to go back for more medicine. This is going to be lucrative for the pharmaceutical company but probably not in the patient’s best interest.”
In Bennett’s clinic, ketamine is administered only alongside talk therapy, which she uses to prepare patients before they take ketamine, and afterward to help them process the experience. “I think this is the only ethical way” to administer a drug that can trigger disorienting psychedelic experiences, she says. “This isn’t a ‘take two and call me in the morning’ situation.”
There’s growing scientific interest in whether ketamine can enhance the effectiveness of therapy by increasing the brain’s ability to remodel circuits through experience, Krystal notes. And in 2017 a small Yale study found that providing cognitive behavioral therapy in tandem with ketamine can extend the drug’s antidepressant effects.
Unlike some researchers and pharmaceutical companies, which consider ketamine’s and esketamine’s hallucinogenic side effects inherently negative, Bennett thinks that for some people the visions can be positive — particularly in the context of therapy. There’s scant scientific evidence to support the idea that such hallucinations are therapeutic, and they can be deeply disturbing for some people. (If people who experience hallucinations do better, it may simply be because they have received a higher dose of ketamine, Krystal points out.)
Still, Bennett thinks researchers and clinicians need to stay open-minded about why ketamine is helping people — and be more attentive to the settings in which ketamine and esketamine are administered. “People consistently report that they experience the presence of God, or their own sacredness,” she says. “When someone comes to my office wanting to kill themselves, ready to die — and then they have a transformational moment where they believe their life is sacred — it’s indescribable how exciting that is as a clinician.”
Editor’s note: This story was updated March 29, 2019, to correct the affiliation of neuroscientist Bita Moghaddam. She is a professor at Oregon Health & Science University.
ABOUT THE AUTHOR Emily Underwood Emily Underwood
Emily Underwood is a freelance science writer and contributing correspondent for Science magazine. She is based in Coloma, California.
CONTENT PROVIDED BY Knowable Magazine Knowable Magazine
Knowable Magazine is an independent journalistic endeavor from Annual Reviews.
This article was written in entirety by Scott Aikins and Clay Mosser, from The Conversation in The Contributor and all links belong to them. All credit to them.
Note; This law passed at the end of November, 2020, but we thought we should put it up here as it’s such a major bit of groundbreaking legislation that who knows what might come next – An American state doing narcotic decrim? Who would have thought?!
Oregon became the first state in the United States to decriminalize the possession of all drugs on Nov. 3, 2020.
Oregon’s move is radical for the United States, but several European countries have decriminalized drugs to some extent.GETTY IMAGES
Oregon became the first state in the United States to decriminalize the possession of all drugs on Nov. 3, 2020.
Those drugs are still against the law, as is selling them. But possession is now a civil – not criminal – violation that may result in a fine or court-ordered therapy, not jail. Marijuana, which Oregon legalized in 2014, remains fully legal.
Oregon’s move is radical for the United States, but several European countries have decriminalized drugs to some extent. There are three main arguments for this major drug policy reform.
1. Drug prohibition has failed
In 1971, President Richard Nixon declared drugs to be “public enemy number one” and launched a “war on drugs” that continues today.
Criminologists find that other consequences of problematic drug use – such as harm to health, reduced quality of life and strained personal relationships – are more effective deterrents than criminal sanctions.null
Arresting, prosecuting and imprisoning people for drug-related crimes is expensive.
The Harvard economist Jeffrey Miron estimates that all government drug prohibition-related expenditures were US$47.8 billion nationally in 2016. Oregon spent about $375 million on drug prohibition in that year.
Not everyone who uses drugs needs treatment. Decriminalization makes help accessible to those who do need it – and keeps both those users and recreational users out of jail.
Freed up from policing drug use, departments may redirect their resources toward crime prevention and solving violent crimes like homicide and robbery, which are time-consuming to investigate. That could help restore some trust between law enforcement and Oregon’s communities of color.
“I think it sends a really bad message to them, and influences their perception of the risks,” James O’Rourke, a defense attorney who helped organize the opposition to measure 110, told the news site OPB in October.
But U.S. states that legalized marijuana haven’t seen adolescent use rise significantly. In fact, marijuana consumption among teens – though not among college-aged Americans – actually declined in some states with legal marijuana. This may be because legal, regulated marijuana is more difficult for minors to get than black-market drugs.
The local government shut down Platzspitz Park. But rather than chase off or arrest those who frequented it, it began offering methadone and prescription heroin to help people with opioid use disorder. Public injection, HIV rates and overdoses – which had all become a problem in Zurich – plummeted.
Certain parts of Oregon already have higher rates of public drug consumption, namely Portland and Eugene. Because public drug use is still illegal in Oregon, however, we don’t expect a Platzspitz Park-style open drug scene to emerge. These places should benefit from the expansion of methadone programs and other medication-assisted treatment, which is endorsed by the American Medical Association.
There are risks with any major policy change. The question is whether the new policy results in a net benefit.
In Portugal, full decriminalization has proven more humane and effective than criminalization. Because drug users don’t worry about facing criminal charges, those who need help are more likely to seek it – and get it.
These policies show that problem drug use is a public health challenge to be managed, not a war that can be won.
This article was written by Scott Akins, professor in the Sociology department at Oregon State University, and Clayton Mosher, professor in the Sociology department at Washington State University, for The Conversation. It is republished here with permission.
Hi folks, I just wanted to share with you a very interesting book a colleague sent to me the other day. Its all about using coca leaves to help treat cocaine dependence. It goes into great detail about this ‘tried and tested’ treatment, looking at cocaine and its alkaloids, its’ uses over the years, and everything you ever wanted to know about coca leaves. useful stuff about freebasing and crack, the reward system and how cocaine works in the brain, and lots of interesting stuff about coca and why and how one can use it as a treatment for cocaine dependence. All in chunks that are easy to read and aren’t overwhelming or dense. (link to the book below).
The book is entitled Brief Review of Oral Cocaine for the Treatment of Cocaine Dependence.’ Written by Luis M. Llosa MD. Obviously, it talks in detail about coca (leaves) and its uses as a treatment. It claims to have been used for hundreds of years in the Andes and that “References of oral cocaine use (as alkaloid) have shown that traditional doses do not produce intoxication, behavioral disorders or lead to addiction
.”“After the digestive absorption of oral cocaine, the concentrations in blood rise slowly in about 10 to 15 minutes. The slower and more sloped peak in blood levels is thought to be responsible for the apparent low rate of addiction of the oral route. The physiological and psychological effects of oral cocaine last twice as long as those when used by aspiration, three times as those used by IV route and five to ten times longer than those when smoked. This gives it many therapeutic advantages: a slow absorption avoiding its accumulation and toxicity, low blood concentrations, low but sensible physiological and psychological effects ”
It was fascinating to read about all the drugs NIDA (National Insitute for Drug Abuse) in the US, have tried and tested to look for answers in how to treat cocaine dependence. I thought you guys would appreciate seeing some of them:
Other substances under investigation in the last years are Nacetylcysteine, Cabergolide, Ondansetron, Diltiazen, Reserpine, Selegiline, Vigabatrin, Oral Cocaine (Llosa 2007; Gorelick 2009)
Phew! That was a mouthful!
The author, Llosa, in 1994, published the results of the first study performed with oral cocaine (as coca tea) to control cocaine addiction. In 1994 Llosa presented the results of the first double-blind trial as agonist therapy performed with oral cocaine as coca tablets Then, in 2005 Llosa & Llosa presented in the CPDD 67th annual meeting the review of oral cocaine as agonist therapy in cocaine dependence. The author concludes that “Orally cocaine contained in coca leaves has been consumed by Andean people for thousand years for work, social and spiritual purposes without users show signs of diseases and behavioral disorders.”
Llosa also contests that “The use of oral cocaine as agonist therapy meets the criteria for substitution (replacement) therapies. The review of the use of cocaine by oral route as agonist therapy has demonstrated efficiency to control cocaine dependence.”
Fortunately, Llosa does tell us how we might use these substances if we had access to coca leaves in sufficient quantities but also describes how they are used (and bought legally) in Peru, for the very same thing. All in all its a great book, a brief review at 28 pages (I think there may be a larger book on sale somewhere?) but I was certain BP readers would be interested in this little gem and it’s all here to download for free!
Thanks to Andres for locating this marvel.
Click this link below for the book Brief Review of Oral Cocaine for the Treatment of Cocaine Dependence
Long time no chat -I apologise, I will not let next year be as slow as this one for blogging, my apologies friends. Today, however, I wanted to let you all know about a really great booklet we have discovered that is free to download and it’s really useful, non-hysterical info for people who are or who know drug users who are also diabetics. Its about managing diabetes when you are an active drug user – something that must actually be very difficult when you consider needing to take meds, needing to eat/avoid certain foods, trying to look after your health when you might not feel like it – or can’t manage it coz you might have other things on your mind, etc.
I really think any diabetic will appreciate this booklet -its full of really interesting information and things I didn’t know anything about. I added a final note at the end of this blog -I felt inspired to do so, so check it out if you fancy it.
(Here is a link to the booklet -repeated at the end of this blog)
Here are a few quotes direct from the booklet and above and below are the links to download the booklet.
The intro goes like this….“Managing diabetes can be difficult to balance with a busy lifestyle or partying. All drug use carries risk. We know that there are people who are diabetic who will choose to take drugs. So we want to highlight some things that can help you to reduce the risk if you do. This information was written by Dr Disorderly – PhD Neuroscience and Immunology. We also collaborated with people who have diabetes and experience of taking drugs.”
Here are some of the tips inside the booklet….
“Eat a meal of long acting carbohydrates before going out.
These include: bread, potatoes, high fibre cereal, oats.
If you are going out for the day remember to eat regular meals – if
food is missed there is a greater chance of a hypo (hypoglycaemic
episode*)
“….Alcohol may cause blood sugars to rise in the short term but will increase the risk of a hypo after the party…”
“….If you are going to a rave or long festival, make sure you
stock up on plenty of sugary drinks and fast acting
carbohydrates to keep in your locker, bag, car or tent…”
“…Never miss insulin doses, however, be extra careful
with taking insulin at the end of the night or just before
going to bed as you are already at risk of having a
hypo from dancing/drinking. In this circumstance, many
people with diabetes will take a reduced dose of
insulin before consuming food and only take a
correction dose if sugar levels are very high, in which
case, they only take a small dose. Ensure that there is a
glucagon kit in the house and that people know how/when
to use it …”
“…Cannabis can lower your blood sugar levels suddenly so make sure you have some fast acting carbohydrates nearby.
And on depressants…. “Avoid eating sugar /carbs to combat lethargy while taking depressant drugs – it could just be the effects of these drugs. Drugs like valium/xanax and can affect your judgement and you might forget to take insulin. Again, set alarms to check your levels and avoid falling asleep without eating carbs. Be aware of taking depressants – it may be difficult for you to recognise the symptoms of a hypo or for others to realise you are experiencing a hypo…”
And even about ketamine, God bless ’em! “The effects of ketamine can mask the signs of a hypo and reduce your ability to treat yourself. If you choose to take ketamine it is essential to check your sugar levels first – especially if it is a big
dose. Set alarms to remind you to check throughout the time you are
taking it as the effects of ketamine could make you forget…”
This is a handy booklet to know about – for drug workers, GPs, drug users, friends and lovers of diabetics and, of course drug using diabetics -especially for those who know little about managing their condition in drug using situations. That must get hard and is worth spending some time really thinking about and researching though I imagine this may be the ONLY booklet out there on this very issue of drug using and diabetes.
Well done to the guys who produced it – Crew: mind altering (also known as Crew2000 and Crew25). These dudes have been around in the UK for a LONG time now and have always produced good information and have lots of great stuff on psychedelics and stimulants. Well worth a visit.
One last word on the subject of our health as active drug users: It’s really important to learn about your own body and how it reacts to taking illicit drugs; ie -do certain drugs make you forget to medicate, do certain foods work better at keeping your levels correct (ie like for how long etc, remember this to list it as a food to take before partying, for example). Like people who have seizures, keeping a diary and noting down what has been really good at keeping you well, while also notingwhat you did when it goes wrong for you -did you miss sleep, what drugs did you take, what foods did you eat and when etc. Take your control back and learn how to live with your illness like a pro. Tell us about your experiences of being a diabetic and a drug user. We think this booklet is great -we need more thinking like this -looking at our health even though we are active drug users. Because WE want to know! We do care about our health (despite how it might look to some) and we want to stay safe when we use our drugs! I know because of all the thousands of enquiries this website gets each month – the top 3 looked at topics looked at every single month year on year are ALWAYS; drug-related seizures, overdoses and abscesses -and, ok, there is how to freebase coke as well that is always rolling about in the top 3 or 4 as well! Well, we are drug users! Yet even that is saying – how do we get the shit out of our cocaine and make it purer. That tells me more of the same -we want to learn how to make better choices whenever we can. We might not always manage it -or even want to -but our good intentions are there and knowledge is power -the more we learn, the more able we become to make those choices as soon as the opportunity arises. Sleep well comrades, stay safe.
Again, apologies for the long absence on the site -I have been involved with some other activism, mainly on the European front, as part of the new EuroNPUD, the European Network of People who Use Drugs, whose aim is to represent the interests of drug users in the EU.
I will try and post more frequently however as BP is very close to my heart and we still have tens of thousands of people accessing the site every month, so thanks for coming back -we need information updated on the site and we have had someone connect with us offering to put the back issues up in PDF format, which would be fabulous as this is yet to be done in full so we will look forward to that.
Anyway, what propelled me to post today was coming across a neat 10min BBC video on the trend of DIY microdosing on acid or mushrooms. In the video they speak with a handful of very interesting people such as Ayelet Waldman who used acid in microdoses to combat her own deep depression, with ‘earth shaking’ results -and she has written about it in a book called A Really Good Day. And the very interesting James Fadiman, who has been researching psychedelics since the 1960’s and now has a website where he discusses microdosing in detail as well as collecting data on those who do it. His website says “This website has information on microdosing, including a protocol many people have used to microdose safely. What we offer is information on safe and effective microdose use. We do that by enrolling people in studies, then recording and analyzing their reports. We then share the results. We also advise and support other research projects related to microdosing“.
So, the piece was interesting, especially in the light of an increase in people microdosing -As James says, “If people are feeling the slightest bit high, then we tell them there dose needs to be reduced”. So it really is about microdosing your dose. We would love to hear from anyone that has done this and what they think about it.
Modafinal -How Smart is a Smart Drug?
Shortly after this video, getting sucked into YouTube (as you do), I came across another one on Modafinal. We really don’t hear a lot about Modafinal these days but it is still out there and this is quite an interesting piece. The young journo actually takes some Modafinal on camera and has tests at a clinic to see if it really improved his cognitive functioning. It did. By 10%. Not a lot but he certainly looked like he was buzzing a bit. But as he says, it wasn’t all plain sailing. Although this film was made before the UK’s crazy Psychoactive Bill, and Modafinal is still legal to buy as long as you don’t sell it, it still gives a rather interesting look at what is a pretty interesting drug…Not quite like a speedball but, hey ho it is still a stimulant. BP would love to hear from you if you have taken Modafinal and let us know what you thought.
So, that’s it for today, I will get back on the case and keep BP updated. In the mean time for those in the EU, have a look at the EuroNPUD website -or indeed the international drug user network INPUD
Introducing a Good practice guide for employing people who use drugs .
A truly indispensable toolkit.
PWUD (People Who Use Drugs) have insights and expertise that can help inform the planning, delivery, monitoring and review of harm reduction and many other drug related services. When we involve PWUD in the design and delivery of services for our community, the overall work becomes more relevant, targeted and accessible. Working in partnership with PWUD helps services to reach and connect with other PWUD more effectively, and importantly, to understand and meet their needs.
A really powerful way of involving PWUD is to employ them as staff.
Employing PWUD sends out a clear message that they are valued partners and are welcome at all levels of service delivery. It also has a very practical set of benefits, helping services to better understand the needs and lived experience of PWUD. PWUD have the right to be employed. Policies that routinely exclude PWUD from the workplace are discriminatory.
This guide has been carefully and thoughtfully written and involved the community of people who use drugs in its design and execution. It provides really excellent information in the form of a practical toolkit that services themselves can and should use when it comes to considering the employment of PWUD’s in services.
It is true, there are unique issues that PWUDs may bring to the workplace if / when employed. However, the really interesting insights, ideas, and approaches a service will experience from engaging PWUDs is sure to make the extra effort of learning how to structure the work environment, all the more worthwhile.
This guide also has really well thought out and evidenced based information for ensuring that PWUDs who are engaged as volunteers or mentors in any service, are able to deliver their very best, and are properly supported and compensated by the service they work hard for.
It is essential that people who are still actively using drugs, and those who are relatively stable in treatment -are recognised as able to make a valuable contribution to the development of our communities drug and alcohol services! It is a field that should not be exclusively for people ‘in recovery’, and as this guide will show, there are many valid reasons why the entire community of people who use drugs all have valuable roles to play in giving us better quality drug and alcohol services.
Here are just some of the topics discussed in this excellent guide. Make sure every drug service is aware of its existence.
2.2. When drug use is a problem (and when it is not)
2.4. Employing ex-drug users and people in recovery
2.4.1. Employing people who are engaged in OST and drug treatment
2.4.2. Employing people who are active drug users
2.4.3. Employing people who are active stimulant users
2.5. The value of staff who use drugs
4.2. Problem drug use and work
4.3. Imposing personal models and philosophies of drug use
4.5. Moving from being a peer to working in a harm reduction organisation
4.6. Inappropriate relationships with clients
4.7. Supplying, or soliciting the supply of, illicit drugs
4.8. When peer support groups become unhealthy
4.9. Managing staff with health conditions that impact on performance
4.10. Managing a death in the workforce or among the client group
Appendix 3: Risk assessment circle
Appendix 5: Examples of job advertisements for staff who use drugs and peer outreach workers
Appendix 6: Model questions for peer interviewers
Appendix 7: Conducting a review meeting
Appendix 8: Developing a self-control programme
Appendix 9: Checklist for managing staff with problem drug use at work
Appendix 10: Training exercises from the Bangkok workshop
Appendix 11: Normal and complex grief reactions
Save yourself a copy and spread it around the staff in the drug services you know -you never know -you might get a job there one day!
NOTE: This guide came out at the end of 2016 and I have written about it before however it was hidden on our website so I thought it should be pulled out again and given a front page showing. I hope you will agree it will be a useful guide for some years to come.
This is a speech spoken at a Remembrance Day event in London yesterday. It gives a personal point of view looking at how the War on Drugs -which is a war on people in every part of the world that has been happening for almost 100 years! Here is just one persons story of being inside this insane maelstrom.
My Name is Anna
My name is Anna and I call myself a drug user activist.
I have been a drug injector for over 30 years and a drug user activist for more than half of that.
In that time – like many of us here today – I have seen a lot of things….
And, like many of us here – I have also had some extraordinary relationships, encounters and random chances with many, many people who used drugs.
People who, for the most part – were not dodgy or crazy – well maybe just a little –
Who were not dirty, lying or cheating horrible people –
But mostly passionate, caring, sensitive and generous people. People who – yes they may have been pushed to the brink –marginalised and isolated by a society that had to criminalise before it cared – judged before it understood; people who should have received better protection from our drug policies – rather than annihilation…..
People who I have loved and cared about, like we all have –and this is why we are here on this very important day today.
As a drug user activist for many years now I have given speeches and presentations at lots of places all over the country –and while every presentation is different – but this one is special.
It is special because this is the one time I can honestly truly stand up and say – loud and proud – how grateful and how fortunate I am to have made friendships with some of the best people in the world – other drug users – fuck – other junkies! – wonderful, courageous people who have often battled huge odds to still be here – today – and many who are literally here today and in this audience.
People who have found each other, often initially through their enjoyment or pain, their that sharing of an illegal substance. You might say prohibition has brought many of us together.
But prohibition has also meant that –many of these very same people – these special, wild and crazy characters – are NOT here today.
Because they are DEAD. Those people –and we all knew someone – who died directly because our insane drug policies continue to make the same mistakes over and over again – day in and day out –while people like I have just mentioned – die!
Think about this: every minute of every day –someones brother or sister is crying out for methadone but cant get it because (like in Russia) they have an idea that it should be kept illegal to stop drug users indulging themselves.
That someones father is being bundled up in a rug in Guatemala and kidnapped by a quazy religious cult who have financially fleeced the relatives by selling a story that incarceration in a blacked out house – against a persons will is the only way to save someone from drugs.
And that – in the filipines a childs mother and father have been shot dead in the street by a vigilante public who cheer the bandits on and tie big signs round their dead necks calling them pushers.
While here in London someones best buddy overdoses alone in a half way hostel because they are using benzos on top of the shitty blackmarket heroin that available in an effort to drown out the misery of life criminalized after yet another prison sentence.
Prohibition is killing our community – over and over, to quickly to count the numbers –only through days like this do we have an opportunity to really reflect on who these policies are really affecting –in real time.
The anger is real – no doubt about that – it is why I became a drug user activist. But I just want to quickly tell you –being an angry activist didn’t happen overnight. It was an accumulation of several lightbulb moments that happened to me – that made me realise – OMG – I do not deserve shit treatment from people and services just because I use drugs and supposedly broke a few rules.
I used to think – well, what could I expect if I did the wrong thing. Jeezus, surely I couldn’t expect to be treated well? I was in the wrong, after all. I didn’t see then that societys label of junkie –and all its connotations – ran so deeply in people – that I was being judged and sentenced by their ignorance.
Ignorance that could literally put my life at risk.
Ill just tell you very quickly about 2 of those litebulb moments:
The first one happened after I had just been diagnosed HIV positive –it was in 1995 and things were different back then –but stigma is stigma and it is still rife today as we know –no matter what its shade or location.
So, 1995, and it was 6 weeks after I had been diagnosed –my first dr appoint. And I went with to this dr appoint –in fact I went with my mum –and I was met by a female dr who proceeded to hammer me, in the most humiliating way, with a series of 100 questions about my drug use, whether I was sharing needles, did I have anal sex –all delivered with the most accusatory tone I was stunned into virtual silence! My mum –after she picked herself and me – metaphorically -off the floor –said ‘excuse me – I don’t appreciate you speaking to my daughter in that way’; and later, after we left and went for coffee, I realized –what she in fact was brimming with –was a judgement: I was guilty, I was a junky, I had brought this on myself. I was the non deserving.
And I realized in a flash: OMG – I had gone to this dr as an open book – as vulnerable as one can be – we both were – I felt like my life was in her hands –and that she didn’t want it. I wasn’t like everyone else – I really was ‘the other’ and this could literally affect my life now.
It was a lightbulb moment.
Later when a friend and I were bemoaning the fact that there were no drug users speaking on world aids day, considering how we had seen its impact on the injecting community; my friend Andrea, had just been telling me about her husband who had just died of aids. How incredibly courageous he was (in fact John mordant was one of several drug user activists in the world who formed the first front line of user activism back in early 1990s.- also started Mainliners) And that it really felt like there was nowhere for people like him to be welcomed, understood, appreciated –like there was for gay men at the time.
She said to me pointedly “ Because we have heroes too”.
And tears started to well up in my eyes because all of a sudden I thought about all the wonderful people I knew, some of whom were now dead –who never got the appreciation, the respect, the support even the funeral they should have got – just because they used an illegal substance.
But as I said – drug user activism helps me to channel my anger, and has helped me to fight back in constructive ways rather than remaining in a self destructive spiral of guilt, confusion, thwarted ambition, rage.
And days like today are an inspiration – to see all the wonderful people I deeply respect here today –and to celebrate the lives of those who –tragically – and for which there really are no words – are not here today –
Thank you all for coming today to remember those who lived life on the edge –in ways we all sometimes dream about doing but don’t dare –
We will keep remembering them all.
Dedicated to Raffi Ballian – a Canadian masterclass of an activist who died of an overdose this year.






 I just wanted to share with you a very interesting book a colleague sent to me the other day. Its all about using coca leaves to help treat cocaine dependence. It goes into great detail about this ‘tried and tested’ treatment, looking at cocaine and its alkaloids, its’ uses over the years, and everything you ever wanted to know about coca leaves. useful stuff about freebasing and crack, the reward system and how cocaine works in the brain, and lots of interesting stuff about coca and why and how one can use it as a treatment for cocaine dependence. All in chunks that are easy to read and aren’t overwhelming or dense. (link to the book below).
I just wanted to share with you a very interesting book a colleague sent to me the other day. Its all about using coca leaves to help treat cocaine dependence. It goes into great detail about this ‘tried and tested’ treatment, looking at cocaine and its alkaloids, its’ uses over the years, and everything you ever wanted to know about coca leaves. useful stuff about freebasing and crack, the reward system and how cocaine works in the brain, and lots of interesting stuff about coca and why and how one can use it as a treatment for cocaine dependence. All in chunks that are easy to read and aren’t overwhelming or dense. (link to the book below). “After the digestive absorption of oral cocaine, the concentrations in blood rise slowly in about 10 to 15 minutes. The slower and more sloped peak in blood levels is thought to be responsible for the apparent low rate of addiction of the oral route. The physiological and psychological effects of oral cocaine last twice as long as those when used by aspiration, three times as those used by IV route and five to ten times longer than those when smoked. This gives it many therapeutic advantages: a slow absorption avoiding its accumulation and toxicity, low blood concentrations, low but sensible physiological and psychological effects ”
“After the digestive absorption of oral cocaine, the concentrations in blood rise slowly in about 10 to 15 minutes. The slower and more sloped peak in blood levels is thought to be responsible for the apparent low rate of addiction of the oral route. The physiological and psychological effects of oral cocaine last twice as long as those when used by aspiration, three times as those used by IV route and five to ten times longer than those when smoked. This gives it many therapeutic advantages: a slow absorption avoiding its accumulation and toxicity, low blood concentrations, low but sensible physiological and psychological effects ”