Here is a story from an incredible activist from back in the day called Peter VanDerKloot. Peter actually fought to keep open one of NYC’s main methadone clinics from closing, by agreeing to put his entire face (and his boyish all-American good looks) onto a FULL PAGE advert in a NYC newspaper, telling people that methadone had saved his life and was saving the lives of hundreds of others and that it just must not be closed down! It wasn’t, and Pete went on to do some fabulous work in the field and, though I don’t know where he is now, we are lucky to have had a few articles from him. Here is one. From issue 2.
When the Black Poppy crew asked me to do a column on the dope scene in the States, it got me thinking about all that’s changed in my time as a dopefiend here in the Belly of the Beast. It’s hard to believe it’s been 15 years since Ron and Nancy Reagan cranked up the heat on the War on [Some] Drugs and sold folks on the idea that invasion of ones home by a SWAT team was something that all Americans had a right to expect. Not that this was the first time our fearless leaders had declared war on a molecule. We’ve been through plenty of chemical warfare in this country, from turn of the century campaigns against cocaine-crazed Black men visually raping Southern belles with their dilated pupils, to drives in the 70s to save pot-head teenage boys from the shame of Dolly Parton-esque breast growth. All along though, it’s been us dopefiends who’ve made up most of the casualties. Hell, we started the century able to buy pure heroin via mail order and now we end it unable to buy dried decorative poppies in the florist’s.
Still, the last two decades have been rougher yet. The powers that be seem to have decided that the solution to unemployment in our post-industrial
The typical sort of NYC_heroin-baggies_ From Graham MacIndoe’s collection, see more in his photographic book, wraps he collected throughout his using days. Fascinating!
economy is to imprison half the population and hire the other half to guard them. At the rate we’re going, we’ll meet that goal soon – as it is, nearly 1% of our adult male population is currently behind bars. No other Western democracy comes close, and when you factor in the effects of spiraling mandatory drug testing, increased police powers, and ever-decreasing privacy, you can bet that that lead will remain unchallenged – even if our right to call ourselves a “democracy” does not.
Here in my hometown of New York City, the dogs have really been loosed on us. The tanks are filled with public beer drinkers and subway fare-beaters, and you can catch a six month bit just for looking cross-eyed at a cop. And yet when it comes down to copping and getting off, the War on Drugs hasn’t made much headway.economy is to imprison half the population and hire the other half to guard them. At the rate we’re going, we’ll meet that goal soon – as it is, nearly 1% of our adult male population is currently behind bars. No other Western democracy comes close, and when you factor in the effects of spiraling mandatory drug testing, increased police powers, and ever-decreasing privacy, you can bet that that lead will remain unchallenged – even if our right to call ourselves a “democracy” does not.
When I first got turned on to heroin, New York was still the dope capital of the world, and “Alphabet City” was still the capital of New York dope neighborhoods. In the days before the real estate interests moved in and the area was declared an extension of the “East Village” and hence suitable for yuppie inhabitation, the streets belonged to us, and you best believe we made the most of it. Block after block of abandoned buildings and vacant lots were commandeered by major dealing organizations. The streets echoed with the cries of the steerers touting the brand names of different bags: “Red Tape!… Seven-Up…ET!!” We’d line up to cop in queues stretching around the corner, kept in place by enforcers with golf-clubs in their fists or pistols in their waistbands who’d order us to have our money ready and fanned out just so — reminding us not to linger post-purchase with chants of “Cop and bop!” Street traffic was heavy too, as the narrow streets were choked with cars with out of state plates down either to supply the driver’s habit or to run a few bundles back for resale.
This was no. 2 in our series; How Do You Take Yours? We looked at Cocaine, and asked the people that used it, how they preferred taking it and why, and gave some useful harm reduction tips for everyone!
This BP article was brought to you by A&E Lifestyles, a BP partnership in drug taking & drug investigating!
While the BP ‘knowledge’ tends to come from hundreds of combined years of experience of opiate, coca use and loads of pharmaceuticals (and that’s just the crew!), these days, drug taking for the enthusiast is changing. It’s broadening out, it’s becoming consumer savvy, it’s becoming mainstream. Nowadays, we aren’t so attached to one drug anymore, it’s a pill for this, then a smoke for that, then a whole pharmacopoeia of drugs for the come downs. We are learning how to use our drugs, we want to know more about them and what they do and what are the safest ways of taking them. The West has created a pill culture – and drugs are out there by the bucket load. This issue, BP looks at cocaine – and A&E are asking you “How do you take your coke?”
freebase -not the same as crack…
Cocaine is used by such a diverse group of people, probably because it lends itself to being snorted, smoked, injected, freebased, chased, chipped, drunk, or blown up an orifice somewhere, and as such, many of us will have a preference of our own. A (of A&E Lifestyles prefers to have it via injection and mixed with brown in a speedball, while E prefers to have the coke first, then the brown!). The emergence of crack has added more dimensions to what the phrase ‘using coke’ actually means. But as anyone who’s had a coke habit will tell you, no matter which way you take it, consistent, regular use of coke/crack can lead to a whole host of problems – the combo of no food, sleep, come down drugs and paranoia can lead to some serious shit , compounded by the potential health problems due to the method by which it’s administered. A&E spoke to a few coke fiends to get their views on using it their way and have collected some good harm reduction tips to remember – whichever way you use it. (This focuses on cocaine in all its guises except crack -although we do look at freebase and smoking tips -crack kinda needs its own article these days!
Here’s a chat with a few of the people doing the biz, day in and day out, they haggle and hassle (and we cough up and complain)…But by and large, dealer’s are just like us, most are just trying to keep their own habits going without resorting to ‘other methods’. Can’t blame them. Dealer’s don’t sit out the front of schools tempting kiddies, they rarely want to sell to a newbie. In today’s world of prohibition and drug habits, dealing to keep your own head above water, is a way of managing day to day. It is the result of drug laws that leave all our drugs to the influences of the black-market. Some dealer’s are a nightmare, some violent, some a complete rip-off. BP says; if you are going to deal drugs -have compassion, take pride, do your best to give a clean product and treat your customers with respect. It shouldn’t have to get down and dirty. See our ‘Dealers Certificate’ and sign up to it. Let’s make the best of it and treat each other well; we are all struggling out there.
Martin (does heroin & crack):
“I wouldn’t call myself a dealer personally, and this very important to me; whether it’s the profiteering aspect or the pushy aspect, to me it makes a difference. I feel I am providing a service – most of my clients are middle class, I see them twice a day, the same faces; My employers you could call business men or drug dealers, but again, its supply and demand. We don’t push drugs onto other people, we don’t go looking for new converts.
I guess I do it out of choice – it suits my lifestyle, I’m paid a salary – I see the guy at the end of the day and get paid up. It doesn’t work on a commission basis like some setups. I use drugs myself so naturally it keeps my habit looked after. I look at it as a proper job, one has to be professional, it entails a hell of a lot from you and the law aspect is also on your mind. Yet sometimes one reaps the benefits and hits the highs, and meets some amazing people along the way. The myth of the user / dealer’s relationship is complex – discovering all the layers within each customer as you get to see them day after day in all manner of situations…It can be tough job.”
Switzerland, courageous, progressive, humane – junkies around the world thank you!
Dudes and Dudettes, around the globe; As I was just about to write an article for the British press on the demise of the much respected ‘British System’ and the diminishing role of the prescribing of legal, pharmaceutical heroin to opiate-dependent people, I came across this article. Published just last year it gives a brief but interesting look at Switzerland’s incredible journey as an innovator and leader in the field of drug treatment. I hope you may find this as interesting as I have.
Many of us will know something of the Swiss Story, but it is never more pertinent than today, to renew these very important discussions about heroin prescribing, standing up loud and proud and showing off the very real successes this approach has decades on, across Europe today. We must take a leaf out of Swiss’s History book and, while fanning the flames of the decriminalization and regulation discourse, we can burn a clear and wide road ahead, devoid of the forest and the trees – out of our dangerously out of control illicit drugs market, and hopefully towards sowing some damn busting seeds at UNGASS 2016, in New York City. Once home to the archetypal junkie!!
Switzerland’s fascinating journey from the experimental Needle Park to the development of the most innovative, effective and publicly supported heroin prescribing clinics now available across the country and even in (2) prisons.
Friends, it is time we celebrated and thanked our Swiss comrades in arms -for their bravery in going it alone for so many years; their refusal to condemn junkies to the gutters and prisons of society, for standing so far out in the crowd in the search for humane and pragmatic solutions to the fallout from prohibition, and all at a time when all around was calling for blood; incarceration, isolation and discrimination.
A street heroin epidemic that was to sweep through Europe and the rest of the world during the 70’s and 80’s, while nations governments used tactics and policies that were brutal at worst -and misguided at best – psychiatrists and medical professionals began years of postulating and aggrandising their professions and their careers.
Article reprinted as it appeared on the online newspaper SWISSINFO.CH
At the beginning of the 1990s, pictures of the open drug scene at the so-called “Needle Park” in Zürich went around the world, leading to the introduction of legal heroin prescribing. Strongly criticized at first, it has since been hailed as an example.
The old Needle Park in Zurich, Switzerland; the experiment that paved the way towards one of the world’s most successful drug policies -heroin prescribing. Click the image to see more pictures of the era in Needle Park.
Doctor André Seidenberg, who has treated 3,500 patients suffering from addictions in his career, was one of the first to provide emergency help in Needle Park and to call for clean syringes to be given out to addicts. Police and the justice authorities tried to deal with the problem with repressive measures that failed to work. The crackdown even encouraged drug addiction and the drug trade, Seidenberg claims.
swissinfo.ch: Twenty years ago Switzerland became the first country to prescribe heroin to therapy-resistant addicts. Has it been a success story?
André Seidenberg: Yes, although you have to bear in mind that the heroin programme has been marginal and to my knowledge never reached more than 5% of the affected people. It is a kind of show project, a prestige project.
It is however a success because in Switzerland, the majority of people dependent on opioids are in treatment, mostly with methadone, and a small proportion, particularly those who respond poorly to therapy, with heroin. It would be preferable if the proportion of addicts in treatment could be increased. I wish we could have gone further with the medicalisation and legalisation of the market.
Needle Park in Zurich today, heroin use is very clearly on the decline
swissinfo.ch: Would that have had an effect on the black market?
A.S.: Of course. The black market is a market that is encouraged by repressive measures and ultimately produces poor products that are harmful to people. I wish we could have a less hypocritical approach to drugs.
swissinfo.ch: Then you are in favour of a general legalisation of drugs?
A.S.: I am in favour of better market control. It is an international problem, because we still have a very active drug wars in many regions.
Appropriate control of the drug market is not a trivial matter either. One cannot for example just legalise cocaine and think that all problems will be swept away. It would have to be introduced very carefully.
swissinfo.ch: How is life different for a person who doesn’t have to seek out heroin in the back streets anymore but receives it regularly as a medicine?
A.S.: A person who receives their fix twice a day is in psychologically better condition, is more stable in every way. Of course there are side effects and even lasting impairments. Those who take this substance daily suffer from decreased libido, sleep problems or a limited capacity to experience emotional states in between euphoria and sadness.
People who take part in a heroin programme are also freed from the necessity to finance their existence through illegal activities. Delinquency, prostitution and social deviance of all kinds have decreased.
swissinfo.ch: So they can lead a normal life?
A.S.: The possibility of procuring drugs in this [legal] way makes a big difference, because in illegally procured drugs tend to be consumed in more dangerous ways. Most addicts are not in a position to always inject themselves carefully, which can lead to infections and infectious diseases. Overdoses also happen much more easily with drugs bought on the street.
When we are able to look after people medically, these risks are avoided to a larger extent. With controlled distribution people are able to lead a mostly normal life, although there are more people getting disability benefit among those taking part in the heroin programme, compared to the methadone programme.
swissinfo.ch: So from a medical point of view the focus is on limiting harm and stability rather than abstinence?
A.S.: The priority for doctors is to avoid serious harm to the body and death. Healing the soul comes, in medical terms, just after the body.
swissinfo.ch: Should abstinence not be the goal of a state drugs policy?
A.S.: That was the goal of politicians and society, and many doctors still nurture this illusion. But it’s a very dangerous strategy. Heroin addiction is a chronic illness. Only a small, shrinking minority of opioid addicts will become abstinent long-term. And most of them suffer during their abstinence.
With heroin – as opposed to alcohol – abstinence doesn’t improve well-being and health. The death rate is three to four times higher for abstinent patients, compared to those prescribed heroin or methadone. Repeated attempts to come off the drugs can trigger psychological difficulties, that can then lead to self-harm.
swissinfo.ch: Is heroin still an issue today?
A.S.: Thankfully we rarely see young people taking up heroin. Consumption has fallen massively. One per cent of those born in 1968, the Needle Park generation, became addicted and many of them died because of their addiction or are largely still dependent.
The average age of a heroin addict in Switzerland is now around 40. If we hadn’t stopped this development at the beginning of the 1990s, young people born in the following years would have been affected to the same extent. There are societies, for example the countries of the former Soviet Union or Iran, where a significant percentage of the population is dependent on opioids.
swissinfo.ch: You tried out various drugs, including heroin. Why didn’t you become addicted?
A.S.: Maybe I was just lucky. When I was young I tried out almost all kinds of drugs. I was able to satisfy my curiosity and maybe also learnt certain things that could be useful for my patients. I also got to know the danger of drugs: I lost many friends, even before my medical studies began.
swissinfo.ch: Do you have to have taken drugs to be a good drugs doctor?
A.S.: No, I would not recommend that. When dealing with problems that have to do with the psyche, it is definitely helpful to have an open mind. But you don’t have to try out everything for that, because that could be harmful and dangerous.
(Translated from German by Clare O’Dea), swissinfo.ch
Swiss drugs policy -A Timeline
Since 1991 Switzerland has implemented the so-called four pillar policy of prevention, therapy, damage limitation and repression.
This pragmatic policy was developed largely in response to the extreme drug-related misery in Zurich in the 1980s and 1990s.
The controlled prescription of heroin was first introduced in 1994.
In 1997, the Zurich Institute for Addiction Research came to the conclusion that the pilot project should be continued because the health and living situation of the patients had improved. There had also been a reduction in crime.
In 1997 the people’s initiative ‘Youth without Drugs‘, which called for a restrictive drugs policy, was rejected by 70% of voters.
In 1998 74% of voters rejected the ‘Dro-Leg’ initiative for the legalisation of drugs.
In 2008 68% of voters accepted revised drugs legislation. Since then controlled heroin distribution has been anchored in law.
The new law came into force in 2010.
Further reading; (docs come in German, French, Italian and English
(from BP Issue 9 but now with new updates as of Nov 2015)
Many BP readers will have already witnessed the distressing sight of someone having a seizure, or you may have even experienced one yourself. It can be frightening to watch, exhausting to go through and unfortunately, people can often make the situation worse by not knowing how to deal with seizures properly, leaving everyone concerned thoroughly freaked out.
Most people associate seizures with having epilepsy and while it is certainly true to say that seizures (there are over 40 different types) are a symptom of having epilepsy, you don’t have to have epilepsy, to have a seizure. Anyone who has seen someone have a cocaine or alcohol induced seizure can attest to that.
Drug Induced:
For those of us who use drugs, particularly those of us who binge use or use to excess, seizures are known to occur for a few reasons. Sometimes they happen just before or as someone is overdosing, (i.e a seizure occurring just in the minutes before someone actually lapses into an overdose) or through withdrawing from a drug/s (i.e benzos, alcohol) or, they are a (rather intense) way of telling us that we have been pushing our bodies too hard for too long (i.e cocaine/stimulant related) and we can have a seizure which although is not an overdose -it is an overdose in the sense that you have reached the threshold in what your body can tolerate -and it is telling you -“Enough! My body has now gone into toxic overload!”. Basically, seizures occur when our systems have reached this point of toxicity or overload, even if the culprit drug is ecstasy, acid or heroin -when we tend to think of the most common culprits as stimulants and alcohol and benzodiazepines and barbituates.
Know Your Limit
Everyone however, has what is called a ‘seizure threshold’, a certain sensitivity to seizures which means that anyone can experience one given the right conditions – such as excess use of alcohol, drug withdrawal, toxicity, dramatic metabolism changes etc. With 1 in 20 people having experienced a seizure at some stage in their lives, amongst drug users that rate increases rather dramatically, so its important that we learn something about seizures, their ‘triggers’ as well as their treatment.
It can be all too common to put the odd re-occurring seizure down to ‘the drugs I’m taking’ or to find that our medical investigations have not been followed up due to the pressures of everyday life and the difficulty embarking on consistent/stable medical care when you have other things on your mind like survival. But it’s important to remember that seizures can be very serious, they are hard work for the body and the brain in particular and, depending on where you are when you have your seizure, or if you end up having multiple seizures, you can be left in a dangerous or vulnerable situation.
If you are affected by seizures, if you have had more than 2 at once or 2 or more during the last year, or if it takes you more than a day to recover, or if your seizures start to occur regularly, it is essential you seek medical advice – at least to rule out any underlying causes such as infection, virus’s, tumors etc. You might have developed epilepsy in which you need medication, or there may be an underlying medical condition that has nothing to do with your drug use. You need to know these answers so you can take the right action.
To read the rest of this interesting and updated article, click here. Comments always welcome
Abscesses are something most of us have encountered before and they can be everything from hardly noticeable, to extremely painful. Medical care can be hard to come by for many of us around the world who inject drugs and so some people resort to treating themselves, for reasons of cost, access, stigma or fear. This can lead to some serious complications as the toxicity of an abscess can vary considerably. Here are a few things to remember when it comes to getting to grips with an abscess -and whether you can really treat it yourself. Yes, you may think you know what to do if you have an abscess, but there is new guidance in terms of treating them these days, to ‘pack or not to pack’ , antibiotics everytime or just some of the time? Yes, this is a big article and has had a major update, and we will edit it down in the coming weeks, but for now here is all the information we have collected to help you make the most important decision -when to get help. Yes, it is worth reading the whole thing if you are concerned about abscesses, or at least read the summary!
A fairly typical large sized infected abscess on a heroin user who is said to have skin popped heroin recently.
This is a pic of an infected abscess, but one where it was only recommended to just cut and drain, and not necessarily dispense antibiotics.
A Sterile Abscess is caused by injecting either an irritating or insoluble substance into a vein – and if some of the cut in your drugs are insoluble, a sterile abscess is sometimes formed. It is basically a milder form of the same process of an infected abscess, caused not by germs this time but by nonliving irritants such as drugs. If an injected drug is not absorbed, it stays where it was injected and may cause enough irritation to generate a sterile abscess—sterile because there is no infection involved. Sterile abscesses are quite likely to turn into hard, solid lumps as they scar, rather than remaining pockets of pus. It will not usually show signs of heat although there may be a touch of redness and it can feel like a solid nodule under the skin and isn’t likely to be sore. Soreness will depend on the volume of substance under the skin. Don’t try to squeeze or poke it as it will usually go away in its own time and squeezing it could induce an infection.
A Septic or an Infected Abscess can occur anywhere in the body. In the injecting community in which we are referring to here, these can be caused by either using non-sterile injecting equipment or by bacteria from your skin entering under the skin via the injecting process. An infected abscess will soon come up as a swollen lump on or near the injection site. Appearing inflamed and red, it feels hot to the touch and soon becomes very painful. The abscess may come to a ‘head’ or ‘point’ and be filled with pus. Sometimes a deep abscess will eat a small channel (sinus) to the surface and begin leaking pus. It can be tempting to squeeze or burst it now – but DON’T! This will only spread the infection, driving it deeper and wider, and it could head for the bloodstream making you very ill by giving you blood poisoning which can be fatal!
Hi again, For all you activists out there, check out this really terrific piece of work from some really interesting collaborators – and all their materials are available for others to use. Really useful stuff on how to explain the issues affecting people with multiple needs so that politicians and policymakers can understand the issues and the people better and thus, should be more able and willing to really listen.
Voices from the Frontline is an “exciting new project to bring the voices of people with multiple needs and those who support them to the heart of the policy debate.” Click here for more info. I love their thinking! Opportunity Nottingham exist to help people fighting at least three of the following: Reoffending, substance misuse, homelessness and mental ill health. “In achieving our primary goal of helping people we are also going to change the way the existing system of support works.” Bloody fantastic! I love this new way people are starting to think regarding issues of homelessness and incarceration, mental health problems and drug use etc; we have developed certain tools of empowerment -now we need to cross that divide, find out how we can make politicians really, but really understand our issues. Places where we can find the common ground, the language; As they say in the notes of what came out of their collaboration, “We need to move away from defensive practice. Services can help people raise their voice, but they’re not really listening if they’re only defending their own position”. So true, so true. Visit these sites my friends, for some really useful tips.
Bye for now – and thanks to the people working so hard to develop these amazing organisations and work towards changing the minds of some of the stubbonist in society – the politicians and policymakers!!
Here is the piece below…
How to build support: frontline tips for influencing politicians and policymakers
Last Wednesday, a number of participants in Voices from the Frontline traveled to the Multiple Needs Summit in London. Over the last few months, all of them have been involved in a conversation about what the next government should do to improve support for people with multiple needs.
A big part of this conversation has been about how to explain the issues affecting them so that politicians and policymakers can understand and will listen. For that reason, we held a joint workshop with Opportunity Nottingham (an organisation improving services for people with complex needs in the city) to explore this.
One thing was clear: there’s a huge amount of knowledge out there about how to put the case across. Here are some of the best tips that people had.
Get the right people in the room, and you’ll get the right answers. Go into a room feeling confident. Get people to listen to what you say (even if they roll their eyes.)
Bring people together and get them to talk about a real case study. Then they’ll realise that languages are different, and there are other worlds they very rarely think about.
Beware of ‘innovation fatigue’. For instance, someone explaining Fulfilling Lives (a major programme to help local areas improve how they work with complex needs) met with people saying “you’re just another person coming to my meetings – we’ll never see you again”.
Sometimes the bad news and bad stereotypes that exist can make it really difficult. It can help to capitalise on them, though. “If I don’t address those stereotypes, we haven’t had a conversation.”
The higher people are up, the less they know about what’s happening down below. Build relationships based on helping them see what’s happening. How do you bring things that don’t work to their attention?
We need to move away from defensive practice. Services can help people raise their voice, but they’re not really listening if they’re only defending their own position.
Be a critical friend. Or, as one person put it, “don’t throw a strop.”
Finally, don’t assume a divide between policy people and lived experience. There can be more overlap in their knowledge and interests than we sometimes assume.
(Should you be interested, you can read all the notes from the workshop here.)
If you want to think about how your own organisation could do more to influence decision-makers, Opportunity Nottingham have produced a brilliant handout summarising some of the things they’ve learned. Feel free to share it with others who you think might find it helpful.
Making Every Adult Matter
Making Every Adult Matter (MEAM) is a coalition of four national charities – Clinks, DrugScope, Homeless Link and Mind – formed to influence policy and services for adults facing multiple needs and exclusions. Together the charities represent over 1600 frontline organisations working in the criminal justice, drug and alcohol treatment, homelessness and mental health sectors.
This was actually quoted straight out of the UK Labour Party Manifesto this week, the only mention of drugs in the whole thing, mind you…very depressing. It sounds like a last minute, late at night before the final draft of the manifesto is due in to head office… “Oh fuck, we forgot to put something about drugs -shit, ummm, lemme just…umm, Ill just put something like,..’We know drug addiction continues to be a major cause of crime'” person 2 says “Just don’t forget to mention legal highs being illegal!'”
“We know drug addiction continues to be a major cause of crime. We will ensure
drug treatment services focus on the root causes of addiction, with proper
integration between health, police and local authorities in the commissioning of
treatment. And we will ban the sale and distribution of dangerous psychoactive
Hi guys, now you know we are always the first to understand that things are complicated and never just black and white and that a junkies relationship with their doctor/s is something pretty unique (we could all write a book right?) and we are not saying we want all prescribing doctors arrested – that is not the point here, and its a very long way from it.
But just like when you scratch at the ugly scab that is the war on drugs and you find governments’ lying, scheming for their own economic ends, even wheeling and dealing in the very drugs they lock thousands of their citizens up for..and you scratch deeper still and you see the roots of these global drug laws rooted in fear and racism, xenophobia and cultural ignorance, economies and GDP’s, total monopolies by companies and the ever larger monolithic pharmaceutical industrys’ that orchestrate and lobby for the very laws they securely tie up ever tighter still, seeking global domination and a pill for everything we could never even imagine we needed one for….- there is certainly no concern for our youth or environment, – …..Well, I thought you might like to read this article that gives some background into the explosion in Oxycontin in the USA today. How big pharma is raking it in, how the doctors are earning billions as well, how USA overdose rates continue to rise and rise year on year, how prisons keep increasing their numbers of paid lobbyists at Capitol Hill to make sure that, although violent crime is, and has gone down (yes that’s right) in the USA for many years now, more and more laws keep getting introduced to ensnare the illegal immigrant, the petty criminal etc, so society can pay for these ‘Titan prisons’ and maintain the jobs within them, in the cities that the bureaucrats would flourish because of these disgusting, concrete jungles of inhumanity..
But let’s just get a glimpse of how big pharma do things – or rather – how little pharma can grow into HUGE pharma, courtesy of the American taxpayer, and another drug dependent generation – paying the ‘Right Man’ this time, not the junkie down the street….
PS – Remember, we don’t always dig the journo’s language when describing people who use drugs, but we will overlook that somewhat for the sake of the piece. Always write in to the editor to challenge their language if you see or feel that oit is inaccurate, sweeping, or causes offence.
(The link to complete article above and at the end of this text – thanks in advance to Mike Mariani – Here is an extract)
The state of Kentucky may finally get its deliverance. After more than seven years of battling the evasive legal tactics of Purdue Pharma, 2015 may be the year that Kentucky and its attorney general, Jack Conway, are able to move forward with a civil lawsuit alleging that the drug maker misled doctors and patients about their blockbuster pain pill OxyContin, leading to a vicious addiction epidemic across large swaths of the state.
A pernicious distinction of the first decade of the 21st century was the rise in painkiller abuse, which ultimately led to a catastrophic increase in addicts, fatal overdoses, and blighted communities. But the story of the painkiller epidemic can really be reduced to the story of one powerful, highly addictive drug and its small but ruthlessly enterprising manufacturer.
On December 12, 1995, the Food and Drug Administration approved the opioid analgesic OxyContin. It hit the market in 1996. In its first year, OxyContin accounted for $45 million in sales for its manufacturer, Stamford, Connecticut-based pharmaceutical company Purdue Pharma. By 2000 that number would balloon to $1.1 billion, an increase of well over 2,000 percent in a span of just four years. Ten years later, the profits would inflate still further, to $3.1 billion. By then the potent opioid accounted for about 30 percent of the painkiller market. What’s more, Purdue Pharma’s patent for the original OxyContin formula didn’t expire until 2013. This meant that a single private, family owned pharmaceutical company with non-descript headquarters in the Northeast controlled nearly a third of the entire United States market for pain pills.
OxyContin’s ball-of-lightning emergence in the health care marketplace was close to unprecedented for a new painkiller in an age where synthetic opiates like Vicodin, Percocet, and Fentanyl had already been competing for decades in doctors’ offices and pharmacies for their piece of the market share of pain-relieving drugs. In retrospect, it almost didn’t make sense. Why was OxyContin so much more popular? Had it been approved for a wider range of ailments than its opioid cousins? Did doctors prefer prescribing it to their patients?
Because there was simply so much OxyContin available for over a decade, it trickled down from pharmacies and hospitals and became a street drug, coveted by teens and fiends and sold by dealers at a premium
During its rise in popularity, there was a suspicious undercurrent to the drug’s spectrum of approved uses and Purdue Pharma’s relationship to the physicians that were suddenly privileging OxyContin over other meds to combat everything from back pain to arthritis to post-operative discomfort. It would take years to discover that there was much more to the story than the benign introduction of a new, highly effective painkiller.
In 1952, brothers Arthur, Raymond, and Mortimer Sackler purchased Purdue Pharma, then called Purdue Frederick Co. All three men were psychiatrists by trade, working at a mental facility in Queens in the 1940s.
The eldest brother, Arthur, was a brilliant polymath, contributing not only to psychiatric research but also thriving in the fledgling field of pharmaceutical advertising. It was here that he would leave his greatest mark. As a member of William Douglas McAdams, a small New York-based advertising firm, Sackler expanded the possibilities of medical advertising by promoting products in medical journals and experimenting with television and radio marketing. Perhaps his greatest achievement, detailed in his biography in the Medical Advertising Hall of Fame, was finding enough different uses for Valium to turn it into the first drug to hit $100 million in revenue.
The Medical Advertising Hall of Fame website’s euphemistic argot for this accomplishment states that Sackler’s experience in the fields of psychiatry and experimental medicine “enabled him to position different indications for Roche’s Librium and Valium.”
Sackler was also among the first medical advertisers to foster relationships with doctors in the hopes of earning extra points for his company’s drugs, according to a 2011 exposé in Fortune. Such backscratching in the hopes of reciprocity is now the model for the whole drug marketing industry. Arthur Sackler’s pioneering methods would be cultivated by his younger brothers Raymond and Mortimer in the decades to come, as they grew their small pharmaceutical firm.
Starting in 1996, Purdue Pharma expanded its sales department to coincide with the debut of its new drug. According to an article published in The American Journal of Public Health, “The Promotion and Marketing of OxyContin: Commercial Triumph, Public Health Tragedy,” Purdue increased its number of sales representatives from 318 in 1996 to 671 in 2000. By 2001, when OxyContin was hitting its stride, these sales reps received annual bonuses averaging over $70,000, with some bonuses nearing a quarter of a million dollars. In that year Purdue Pharma spent $200 million marketing its golden goose. Pouring money into marketing is not uncommon for Big Pharma, but proportionate to the size of the company, Purdue’s OxyContin push was substantial.
Boots on the ground was not the only stratagem employed by Purdue to increase sales for OxyContin. Long before the rise of big data, Purdue was compiling profiles of doctors and their prescribing habits into databases. These databases then organized the information based on location to indicate the spectrum of prescribing patterns in a given state or county. The idea was to pinpoint the doctors prescribing the most pain medication and target them for the company’s marketing onslaught.
That the databases couldn’t distinguish between doctors who were prescribing more pain meds because they were seeing more patients with chronic pain or were simply looser with their signatures didn’t matter to Purdue. The Los Angeles Times reported that by 2002 Purdue Pharma had identified hundreds of doctors who were prescribing OxyContin recklessly, yet they did little about it. The same article notes that it wasn’t until June of 2013, at a drug dependency conference in San Diego, that the database was ever even discussed in public.
purdue_reformulated_oxy_Pic – crushed by a mortar n pestle: reformulated to deter injecting…
Combining the physician database with its expanded marketing, it would become one of Purdue’s preeminent missions to make primary care doctors less judicious when it came to handing out OxyContin prescriptions.
Beginning around 1980, one of the more significant trends in pain pharmacology was the increased use of opioids for chronic non-cancer pain. Like other pharmaceutical companies, Purdue likely sought to capitalize on the abundant financial opportunities of this trend. The logic was simple: While the number of cancer patients was not likely to increase drastically from one year to the next, if a company could expand the indications for use of a particular drug, then it could boost sales exponentially without any real change in the country’s health demography.
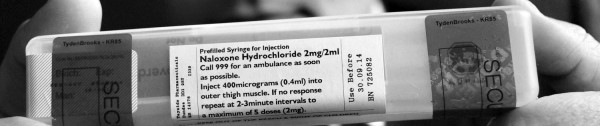
Id like to discuss a campaign involving many members of the drug using community across the world. As far as campaigns go, this one should be a done deal. In fact it should of been snapped up as a central component in all our national and community drugs strategies years ago. The benefits and results to be reaped from rolling out similar campaigns is nothing less than saving life itself and the prevention of repeated tragedy, trauma, gut-wrenching grief and endless pain and loss. What is the campaign? To get Naloxone, the drug that instantly brings a fully overdosed and dying person back to life in seconds, into the hands of every single heroin user and ideally, into the hands of their family and partners.
The reasons to implement and progress this campaigns’ agenda are, at first glance so crystal clear, so straightforward, so blindingly obvious that the average person could be forgiven for asking, “Just what is taking so long? – We need to empower people to save lives, naloxone works, its cheap and simple to use, so let’s do this!”
But, after we remove the blindingly obvious common sense and our societies desperate need to rollout these programmes in the face of rising overdose figures, we must question why we still have unacceptable dithering by authorities and a worrying lack of will to progress the agenda.
It must be considered that such delays carry the familiar hallmarks of the common ‘junkie stain’ or rather, the agenda that is stained or dismantled or even left to rot, simply through its association with drug users. However, this particular campaign, which has come in all sorts of shapes and guises, is gaining traction in areas all over the world and recently, finally, here in the UK too. It has the fangs of drug user activists in it all over the place, with programmes that are getting naloxone into the trained hands of policemen and women, family members and partners, pushing forward the idea of Naloxone as a free item or a purchase from a pharmacy by people, even bringing a used one back to get a new one etc.
There is bound to be something you can do in your own community to help push this agenda forward and to get Naloxone into the trained hands of at least every single heroin user in your neck of the woods, in the rollout towards Naloxone being in every hand, in every city across the world.
What do we do with a medicine that prevents certain death for people with a particular condition—and is safe, cheap, and easy to administer?
Immediately make it accessible to those who can administer it when such a life-or-death situation arises.
Make it available to no one except doctors and emergency room workers.
Endlessly debate the particulars of how and when it should be widely introduced.
If you picked number one, that would seem to be a reasonable choice. Unfortunately, it would also be incorrect. With few exceptions, answers two or three apply in the vast majority of the world when it comes to the medicine naloxone.
Overdose remains a leading cause of death among people who use drugs, particularly those who inject. Increasing the availability and accessibility of naloxone would reduce these deaths overnight.
Naloxone is an effective opioid antagonist used to reverse the effects of opioid overdose. On a global scale, however, exactly how and where naloxone is used remains unclear. International Doctors for Healthier Drug Policies (IDHDP) is seeking to learn why this is and what can be done to change it.
Some form of community-based distribution programs for naloxone exist in over a dozen countries. But the quality of data pertaining to how naloxone is used is highly variable. Enhancing our knowledge about the use of naloxone will help us to better reap its benefits.
What we do know is that the availability of naloxone is growing in several countries. Scotland implemented a national program in 2010, and outcomes there have demonstrated its effectiveness in reducing drug overdose deaths. In China, it is available in an increasing number of hospitals. Canada and Estonia have pioneered programs on take-home naloxone.
And in the United States, policymakers called for greater availability and accessibility of naloxone after opioid overdose deaths more than tripled between 2000 and 2010. In some states, distribution expanded from emergency rooms, paramedic services, and needle-exchange programs to police stations. In Quincy, Massachusetts, all police began carrying naloxone [PDF] in 2010, leading to a 70 percent decrease in overdose deaths.
The role of naloxone in addressing opioid overdose was recognized for the first time in a high-level international resolution in March 2012. Members at the UN’s 55th commission on Narcotic Drugs unanimously endorsed a resolution promoting evidence-based strategies to address opioid overdose. Recently, the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) published a very useful literature review of the effectiveness of take-home naloxone.
To build on these gains, we need more data. IDHDP wants to find more out about the availability and accessibility of this life-saving intervention. To that end, we’ve created the Global Naloxone Survey, an attempt to compile information about where naloxone is available, who can use it, and where it can be accessed with or without a prescription.
We then will analyze the results with the short-term goal of obtaining as much information as possible on how widely and readily available naloxone is. Subsequently, we intend to work to maximize both the availability and the accessibility of naloxone, particularly to those who are most likely to be present where and when an opioid overdose takes place.
This talk on Naloxone was given at a local TEDx event, produced independently at one of the TED Conferences. In 2011, fatal drug overdoses in the UK (3,338) exceeded the number of road accident deaths (1,960). These deaths are preventable. Jamie Bridge talks here about how rethinking both product design and service design have the potential to save lives in the administration of overdose medication. Naloxone was developed in the 1960s to counter the effects of heroin overdose. It’s a staple part of ambulance crew kits, but those who need it face barriers to the drug at the point at which it could save their lives. Recently, there has been a shift in focus and design to ensure that naloxone is available to those likeliest to witness an overdose – drug users, their families and friends. The evidence shows that naloxone works, and that drug users can be empowered to save the lives of their friends.
Jamie Bridge is a passionate advocate for drug services and drug policy reform in order to protect the rights, health and well-being of vulnerable people around the world.
* Naloxone is the generic term, it is also known by its brand name which is Narcan.